Our Otoacoustic Emissions (OAEs) test procedure
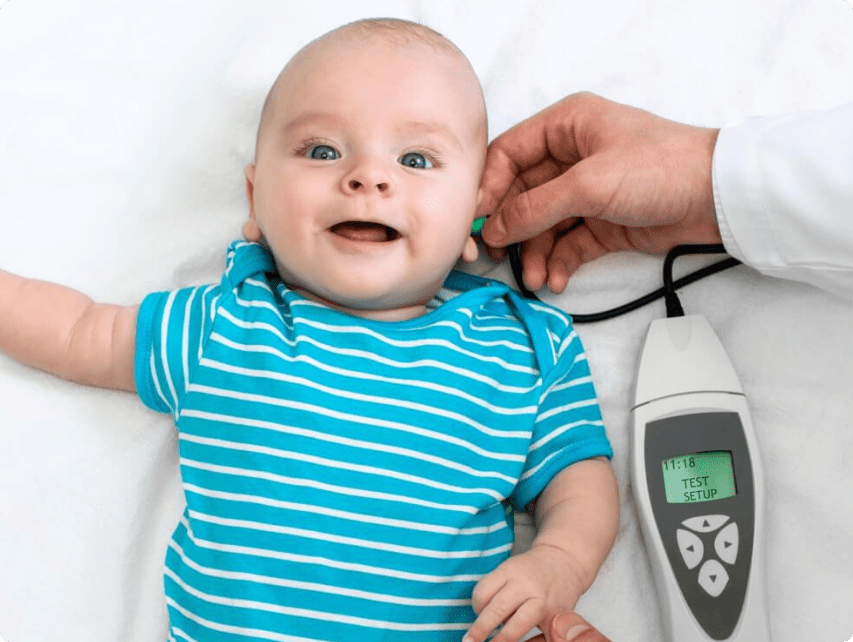
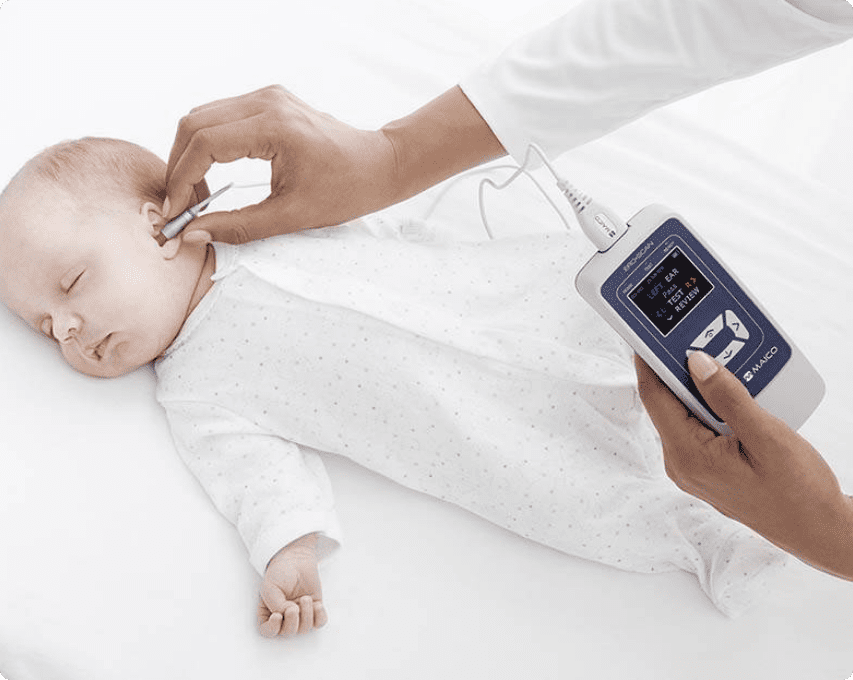
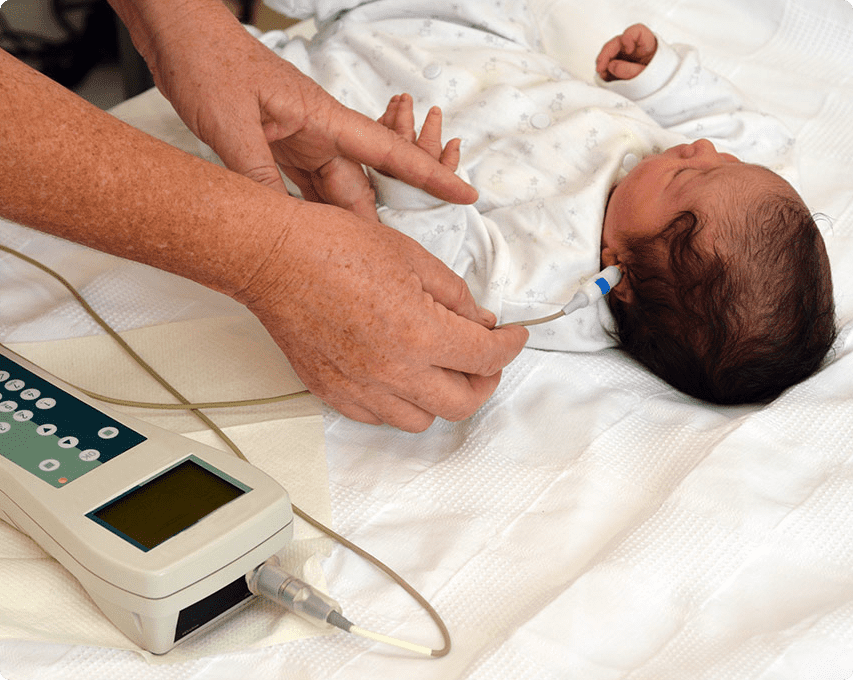
Otoacoustic Hearing testing is non-invasive, and many new-borns fall asleep. Small ear probes are used. The one is a microphone, while the other is a speaker.
The cochlea should echo in response to the sound. The cochlea produces four sorts of sounds:
- Spontaneous acoustic emissions – the cochlea spontaneously creates these noises (not responding to another sound). These occur in 40-50% of persons with normal hearing.
- Transient otoacoustic emissions – created by another brief sound (transient). Sometimes clicks or tones. These are widely used to test baby hearing.
- Otoacoustic emissions as a distortion product – created in response to two simultaneous tones of different frequencies. This helps identify cochlea damage early on (for example, damage to the cochlea from ototoxicity or noise-induced damage).
- Otoacoustic emissions with a sustained frequency are generated in response to a continuous tone. These are seldom utilized in therapeutic settings.
Conditions may induce OAE deficit. Cysts, external otitis (swimmer’s ear), stenosis (abnormal middle ear pressure), perforated eardrum, otosclerosis, cholesteatoma.
Accuracy of Results
It cannot diagnose hearing loss or deafness. To discover whether you have hearing loss, you must pass the OAE exam.
Baby’s with fluid in their ears or other factors that lead them to fail the test even if they do not have permanent hearing loss might cause OAE testing to be erroneous. Other variables that might affect OAE testing results include:
- Poor ear probe seal
- Insufficient ear wax obstruction precludes proper ear probe seal.
- Debris in the ear canal
- A difficult patient
Otoacoustic emission (OAE) examinations are done by our hearing experts to detect cochlear conditions, particularly hair cell function.
Who Should Have an OAE Test?
New-borns should be tested for deafness using OAE. This kind of testing is typically included in newborn hearing screening programs. Otoacoustic emissions testing may also help determine hearing sensitivity. OAE testing is sometimes combined with other tests to look for functional or non-organic hearing loss. This form of hearing loss is difficult to detect due to various probable causes and contributing variables.
Detecting Sounds
A healthy cochlea makes four distinct sounds. Spontaneous acoustic emissions occur naturally without sound. Transient otoacoustic emissions respond to brief noises. Two sound sources create soft echoes with varied tones called otoacoustic emissions. Responses to sustained tones are otoacoustic emissions. The absence of otoacoustic emissions may be caused by:
- Swimmer’s ear
- Middle ear pressure abnormalities
- Cysts in the ear or ear canal
- Eardrum injury
- Anomalies of the middle ear (otosclerosis)
Hearing loss or deafness cannot be diagnosed solely based on the results of otoacoustic emissions testing. Even if a patient fails an OAE test, data from speech, auditory brainstem response (ABR), pure-tone, and middle ear tests are sometimes used to understand their hearing health better. It is especially true when infants or new-borns are OAE tested since being fussy during the test can affect results, as can having a fluid build-up of earwax in the ears.
Ototoxicity Monitoring
It is vital to examine youngsters and others who may not feel well due to therapy with OAEs since they are rapid. OAEs are also cheap. Further testing may be deferred unless OAE testing indicates a need for it. The main drawback of OAEs for this demographic is their sensitivity to middle ear dysfunction, which is frequent in youngsters and immunocompromised people. OAEs are utilized for ototoxicity monitoring, although seldom alone. A shift in OAEs between tests indicates the need for additional conventional and HFA testing.
Using OAEs in Differential Diagnoses
The use of OAEs to help diagnose retrocochlear disorders is now commonplace. OAEs are derived from the peripheral auditory system. Hence they should be present in retrocochlear disease. The internal auditory canal and posterior fossa include neoplasms that might obstruct blood flow to the cochlea. It will influence OAEs. Various studies demonstrate that over 20% of individuals with retrocochlear disease have normal OAEs (Hall, 2000).